
- Acne
- Actinic Keratosis
- Aesthetics
- Alopecia
- Atopic Dermatitis
- Buy-and-Bill
- COVID-19
- Case-Based Roundtable
- Chronic Hand Eczema
- Chronic Spontaneous Urticaria
- Drug Watch
- Eczema
- General Dermatology
- Hidradenitis Suppurativa
- Melasma
- NP and PA
- Pediatric Dermatology
- Pigmentary Disorders
- Practice Management
- Precision Medicine and Biologics
- Prurigo Nodularis
- Psoriasis
- Psoriatic Arthritis
- Rare Disease
- Rosacea
- Skin Cancer
- Vitiligo
- Wound Care
Article
Coding highlights of 2005 & 2006
Year 2005 was filled with many changes that affected dermatologists and how they billed Medicare and other commercial carriers. Year 2006 is anticipated to be an equally challenging year. In this article, I will highlight what I feel was important this year and what you need to be aware of in the year ahead. Due to the space constraints of this article, I cannot go into great detail, but I will at least let you know what you should be aware of and what you need to implement.



Major changes for 2005: A review
1. Mohs requires CLIA Type 1, 2 or 9 certification for billing
b. Claims without the proper certification will be denied.
c. Where does the CLIA number go? Your CLIA number goes into block 23 of the CMS-500 form.
2. Billing purchased diagnostic services based on locality.
Effective January 25, 2005, physicians must bill their local carrier for all purchased diagnostic tests/interpretations, regardless of the locations where the service was furnished.
The billing physician/supplier must ensure that the physician/supplier that furnished the test/interpretation is enrolled with Medicare and is in good standing (e.g., the physician /supplier is not sanctioned, barred or otherwise excluded from participating in the Medicare program).
3. New Medicare drug reimbursement rates.
Effective January 1, 2005 biologicals will be paid based on an ASP (average sales price) plus 6 percent formula. Physicians will be paid based on the allowables (the ASP plus 6 percent) or the actual amount billed on the claim, whichever is lower.
4. Ordering versus supervising provider needs to be on claim.

There are many cases when one physician in the group may order a service, while another member of the group is on site when an NPP, PA or other staff actually performs the service. In these instances, the ordering versus the supervising physician must be identified separately on the claim form.
Simple summary for completing the ordering versus supervising physician CMS-1500 form
Solo practice: If there is only one provider in the practice, then:
a. Item 17 = Provider's full name
b. Item 17a = Provider's UPIN
c. Item 24k = Provider's PIN
d. Item 31 = Signature of provider
e. Item 33 = Provider's practice name, address, zip code, phone number and PIN.
Group practice: In a group practice, the CMS-1500 claim form must distinguish between and identify the ordering provider and the supervising provider. Based on that information you bill:
a. Item 17 = Ordering provider's full name.
b. Item 17a = Ordering provider's UPIN.
c. Item 24k = Supervising provider's PIN.
d. Item 31 = Signature of supervising provider.
e. Item 33 = Group practice name, address, zip code, phone number and PIN.
What to Expect in 2006
1. New hyperhydrosis codes introduced in 2006 CPT book. The new CPT codes are:
64650 Chemodenervation of eccrine glands; both axillae.
64653 Chemodenervation of eccrine glands; other area(s) (e.g., scalp, face, neck), per day.
(Report the specific service in conjunction with code(s) for the specific substance(s) or drug(s) provided).
(For chemodenervation of extremities (e.g., hands or feet), use 64999).
National average Medicare reimbursement for CPT codes 64650 and 64653
will be $48.96 and $66.20 respectively.
General guidelines
a. The J-code for Botox is J0585 which is billed in addition to the injection code(s).
b. The E/M visit can be billed in addition to the injection and J-code if a significantly and separately identifiable service is performed. Modifier 25 must be appended to the E/M visit.
c. These two codes have 0 days in the postoperative time period.
d. These codes are not billed in units. Only one code (e.g., only one CPT code 64650 and one CPT code 64653) can be billed per day (e.g., per patient encounter).
2. Massive coding changes introduced in 2006 CPT Book
In addition to the hyperhydrosis codes introduction, there are new codes, many deleted codes, code revisions, and many additions to the coding instructions for many major categories. Important changes include:
a. E/M inpatient consultations and confirmatory consultations have been deleted. (CPT codes 99261 to 99263 and 99271 to 99275 have been deleted.)
b. Nursing facility visits were deleted; these include CPT codes 99301 to 99303. The new CPT codes are 99304 to 99310.
c. Domiciliary, rest home and assisted living visits changes include the deletion of CPT codes 99321 to 99323. The new CPT codes include 99324 to 99337.
d. New skin graft, skin replacement surgery and skin substitutes codes include vast changes.
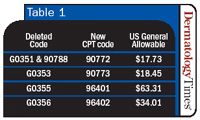
e. New injection codes include the deletion of G0351 (subcutaneous or intramuscular injection) and G0355 (intra-arterial) which are now replaced with permanent CPT codes 90772 and 90773 respectively. The cross walk includes (see Table 1):
3.ICD-9-CM changes
There were no changes on either date that affected the specialty of dermatology on either April 1 or October 1 of 2005. Code additions and revisions are effective on those dates with no 90-day grace period. A complete list of the codes published effective October 1, 2005 are available in Medicare Claims Processing Transmittal 591 by accessing the following web site: http://www.cms.-hhs.gov/manuals/pm_trans/R591CP.pdf
4. Health professional short area modifier change.
Effective January 3, 2006, physicians who have practices in health professional shortage areas (HPSA) will have to use a new modifier to bill to Medicare for their services. For dates of service on or after January 3, 2006, modifiers QB and QU will no longer be recognized. The two modifiers will be replaced by a new modifier, AQ.
Newsletter
Like what you’re reading? Subscribe to Dermatology Times for weekly updates on therapies, innovations, and real-world practice tips.


















