
- Acne
- Actinic Keratosis
- Aesthetics
- Alopecia
- Atopic Dermatitis
- Buy-and-Bill
- COVID-19
- Case-Based Roundtable
- Chronic Hand Eczema
- Drug Watch
- Eczema
- General Dermatology
- Hidradenitis Suppurativa
- Melasma
- NP and PA
- Pediatric Dermatology
- Pigmentary Disorders
- Practice Management
- Precision Medicine and Biologics
- Prurigo Nodularis
- Psoriasis
- Psoriatic Arthritis
- Rare Disease
- Rosacea
- Skin Cancer
- Vitiligo
- Wound Care
Publication
Article
Dermatology Times
Melanoma management perspectives vary
Author(s):
There are many different aspects to the treatment and management of primary melanoma, but clinicians differ on their perceptions of the ideal treatment approach.


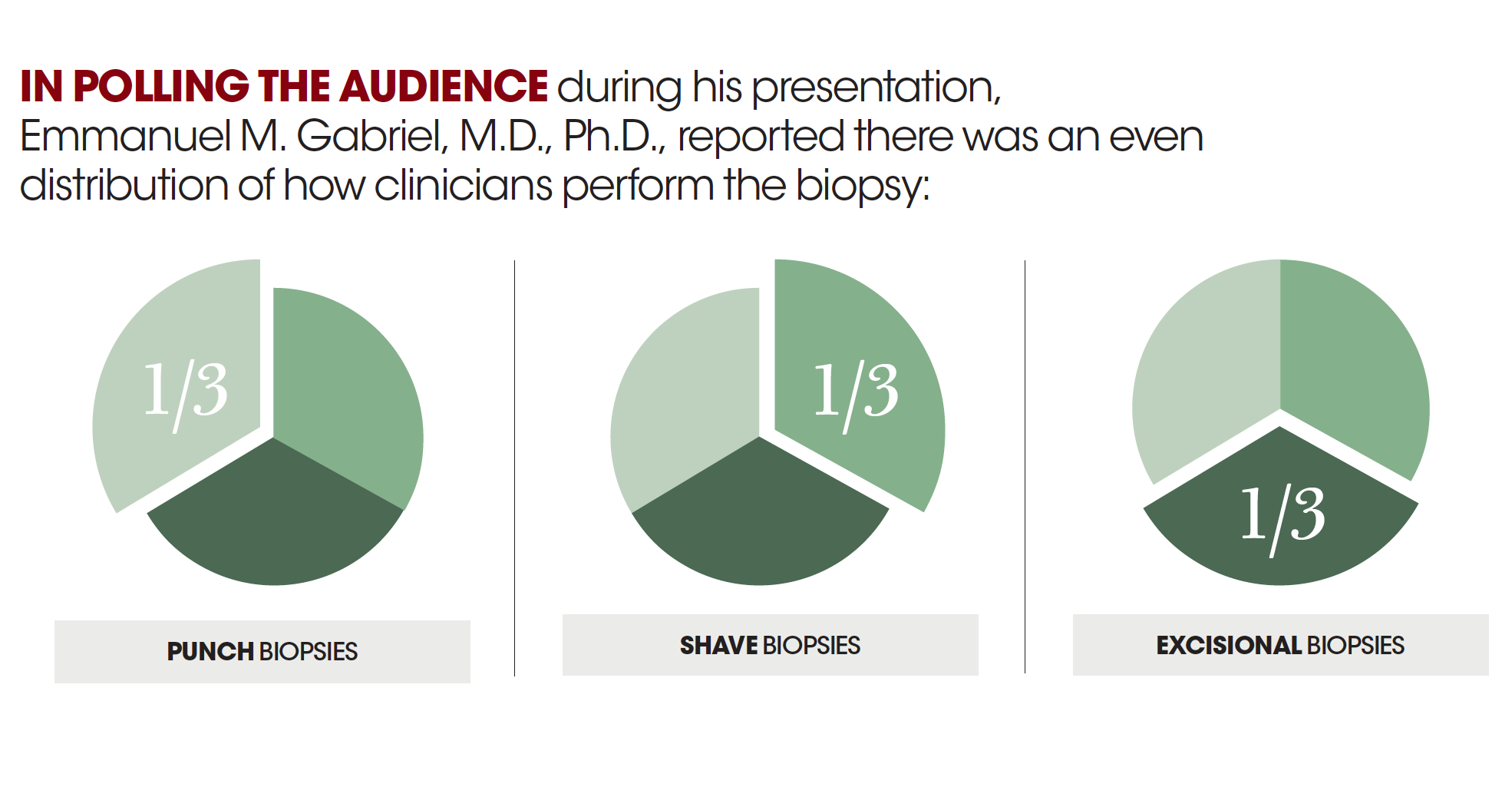
In polling the audience during his presentation, he reported there was essentially an even distribution of how clinicians perform the biopsy, with 1/3 doing punch biopsies, 1/3 doing shave biopsies, and 1/3 doing excisional biopsies.

Dr. Gabriel
There are many different aspects to the treatment and management of primary melanoma, but clinicians differ on their perceptions of the ideal treatment approach.
“Unfortunately, there is no real consensus on several different aspects of the management of the primary melanoma lesion. Many of the recommendations from the National Comprehensive Cancer Network (NCCN) are vague, leaving much up to the interpretation of the clinician and reliance on their training,” says Emmanuel M. Gabriel, M.D., Ph.D., senior associate consultant, section of surgical oncology, department of general surgery, Mayo Clinic, Jacksonville, Fla., who spoke at the 4th Annual Mayo Clinic Cutaneous Oncology Symposium in Orlando.
RELATED: Head and neck melanoma characteristics
There are a number of different techniques that the clinician can choose from to biopsy malignant melanoma including punch and shave biopsy procedures. According to Dr. Gabriel, analysis of the National Cancer Database (NCDB) indicates punch biopsies are more favorable with approximately 60% to 65% of clinicians opting to use this technique. This is closely followed by shave biopsies.
In polling the audience during his presentation, he reported there was essentially an even distribution of how clinicians perform the biopsy, with 1/3 doing punch biopsies, 1/3 doing shave biopsies, and 1/3 doing excisional biopsies.
Although there is no survival benefit associated with biopsy technique, Dr. Gabriel says the choice of procedure is very important to optimizing the further management of the patient.
Shave biopsies, for instance, can potentially impact the downstream surgical planning of the patient. Choosing the appropriate biopsy technique with some foresight for the future surgical procedure would be advantageous, Dr. Gabriel says, as it can affect surgeons later on when addressing wound closure, particularly in terms of how much tissue needs to be removed.
“If a patient comes in with a shave biopsy on a melanoma, typically we are going to perform a wide local excision based on whateverscar is left over. So, the choice of biopsy technique impacts how we are going to close the wound afterwards,” Dr. Gabriel says. “We can potentially have less tissue resected following a punch biopsy, which may have a critical aesthetic role for the patient depending on the location of the primary tumor.”
RELATED: Mechanisms driving melanoma immunotherapy
One of the main controversies among the currently used excision techniques for melanoma is Mohs surgery. Although the technique is considered more for melanoma in situ, Dr. Gabriel says, the NCCN and the Society of Surgical Oncology (SSO) do not support the procedure for invasive melanoma.
“There are trials that are incorporating different margins for certain T stages of tumors, and clinicians are currently using the Mohs technique in certain cases. However, although there are retrospective studies reporting equivalent outcomes of Mohs to wide local excision, it is still not level one evidence. In the absence of prospective trials, Mohs is not generally endorsed for the treatment of primary invasive melanoma for now,” Dr. Gabriel says.
And, when polled for how they would remove the primary lesion, 85% of attendees at Dr. Gabriel’s presentation chose wide excision, he says.
The main reason for the lack of support of Mohs for invasive melanoma is that one of the aims of the excision is to remove the dermal lymphatics where the tumor can spread down and metastasize to the regional lymph nodes. The current guidelines put forth by the NCCN recommend margins to include the dermal lymphatics, Dr. Gabriel says, with the goal of preventing local recurrence and detecting possible satellite or in-transit disease.
“A primary goal of the excision is to prevent a local recurrence,” he adds.
RELATED: What's new in melanoma treatment?
Navigating through the different closure techniques and choosing the most appropriate procedure for the individual case can be challenging. In the end, however, Dr. Gabriel says the choice of closure technique will heavily depend on personal preference of the patient and the training of the clinician.
Skin grafts are very attractive because it is an immediate closure; however, the aesthetic outcome may be less than optimal due to the resulting permanent depression, which is an aspect that Dr. Gabriel says many patients do not immediately recognize.
“Closure through secondary intention, particularly over boney surfaces may be more cumbersome for patients, because they have to be followed up more frequently, but the final cosmetic results may be better than skin graft outcomes,” Dr. Gabriel says.
A lack of consensus over specific surveillance guidelines also remains one of the central issues in the management of early stage primary melanoma. Just how often the patient should be followed up, or whether the surgeon, dermatologist, or primary care physician should take care of the patient during that follow-up period largely remains a grey area. There is no one right answer when looking at surveillance guidelines, and according to Dr. Gabriel, clinicians should perform this in an appropriate way and follow the supported guidelines found in the literature.
“Physicians should rely on their training, and with a multi-disciplinary approach, they can arrive at the most appropriate treatment and management plan for the individual patient,” Dr. Gabriel says.
















Newsletter
Like what you’re reading? Subscribe to Dermatology Times for weekly updates on therapies, innovations, and real-world practice tips.

















