
- Acne
- Actinic Keratosis
- Aesthetics
- Alopecia
- Atopic Dermatitis
- Buy-and-Bill
- COVID-19
- Case-Based Roundtable
- Chronic Hand Eczema
- Drug Watch
- Eczema
- General Dermatology
- Hidradenitis Suppurativa
- Melasma
- NP and PA
- Pediatric Dermatology
- Pigmentary Disorders
- Practice Management
- Precision Medicine and Biologics
- Prurigo Nodularis
- Psoriasis
- Psoriatic Arthritis
- Rare Disease
- Rosacea
- Skin Cancer
- Vitiligo
- Wound Care
Publication
Article
Dermatology Times
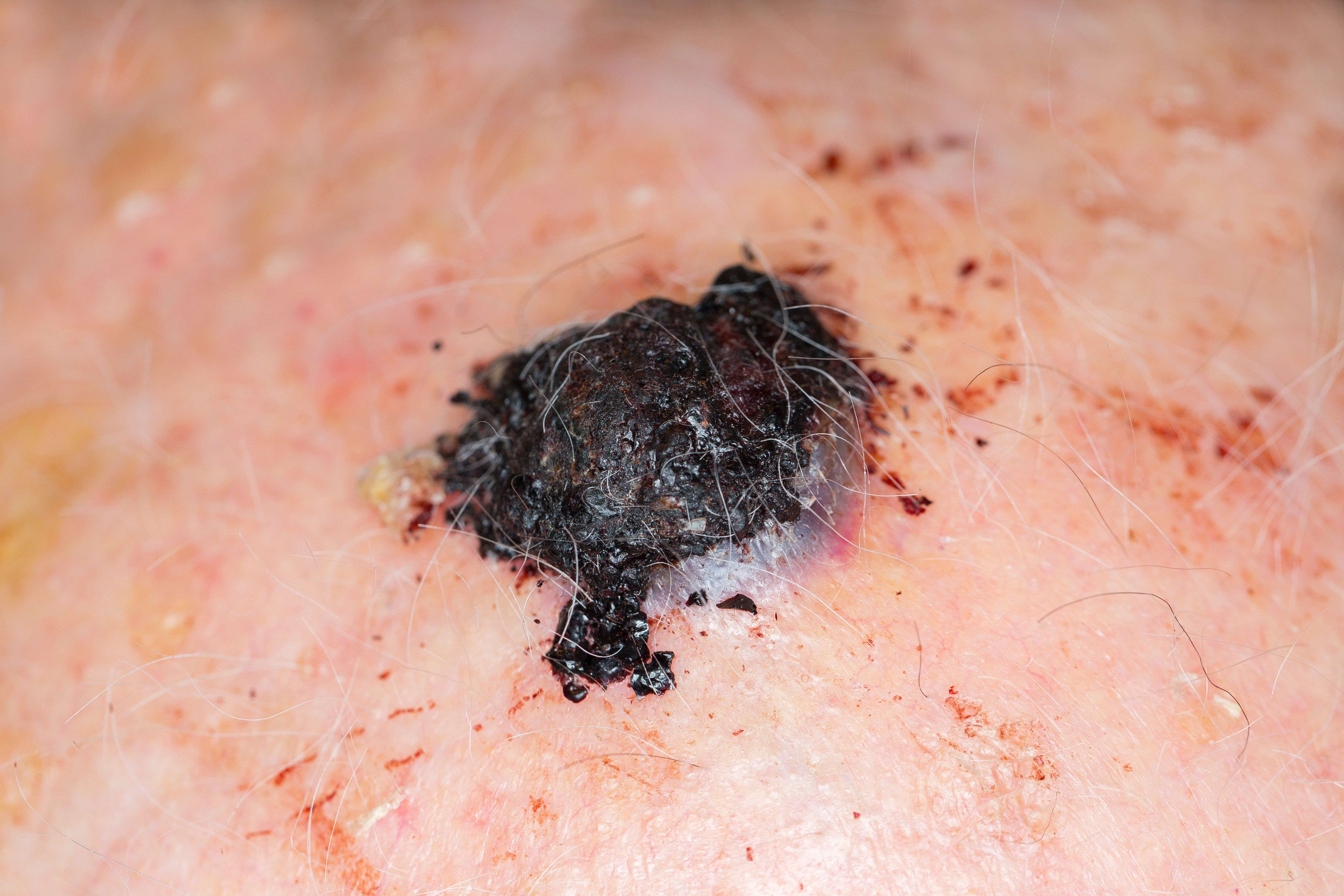
Medical therapy for advanced melanoma
Author(s):
Use of systemic therapies for treatment of melanoma is growing, and so is the list of cutaneous side effects associated with their use.



Dr. Bolognia

Systemic therapies for melanoma were first approved for the management of stage IV disease. Subsequently, several agents gained an indication for use as adjuvant therapy for stage III melanoma, and some therapies are now being investigated for high-risk stage II disease.
RELATED: Standard of care for primary cutaneous melanoma evolves
Although treatment of melanoma with these systemic therapies in the United States is mostly directed by medical oncologists, dermatologists are important collaborators because treatment-related adverse events include a range of cutaneous reactions, says Jean Bolognia, M.D.
She also points out that in addition to their broadening use for treating melanoma, immune checkpoint inhibitors are being used to treat a litany of other cancers. The list of cutaneous side effects associated with their use is also growing.
“Early identification and appropriate management of these cutaneous side effects will allow patients to remain on effective treatment for their cancer. In addition, knowledge of systemic side effects is important so we can discuss them with our patients, especially as immunotherapy is being considered for patients with earlier stages of melanoma who have a better long-term prognosis,” says Dr. Bolognia, professor of dermatology, Yale University, New Haven, Conn.
THERAPEUTIC OPTIONS
Given the multiple systemic therapies that have been approved over the past several years, it is helpful to broadly divide them into two categories: the kinase inhibitors and the immune checkpoint inhibitors.
The kinase inhibitors are further subdivided into two groups:
- the selective BRAF inhibitors, which include vemurafenib, dabrafenib, and encorafenib,
- and the MEK inhibitors, which include trametinib, cobimetinib, and binimetinib.
The most common cutaneous side effects associated with the selective BRAF inhibitors include morbilliform or scarlatiniform exanthems, photosensitivity reactions (in particular with vemurafenib), and keratoacanthomas and squamous cell carcinomas (SCCs). However, the incidence of the latter side effect is markedly reduced when the selective BRAF inhibitor is combined with a MEK inhibitor, Dr. Bolognia says.
RELATED: No-cost BRAF test aids therapeutic decision making
“Palmar and/or plantar fibromatosis is a lesser known cutaneous side effect of vemurafenib that dermatologists need to recognize,” she adds. “Clinicians should also note that they may be the first to describe a novel side effect of systemic cancer therapies.”
The immune checkpoint inhibitors include the anti-CTLA-4 antibody ipilimumab and the anti- programmed cell death-1 protein (PD-1) antibodies nivolumab, pembrolizumab, and cemiplimab-rwlc.
The first three antibodies are used to treat melanoma as well as a number of carcinomas while the latter is approved for metastatic cutaneous SCCs. Immune checkpoint inhibitors that target the programmed death-1 ligand 1 (e.g. atezolizumab, avelumab, duravalumab) have been approved to treat several malignancies including non-small-cell lung cancer.
The three immune checkpoint inhibitors used to treat melanoma differ in clinical efficacy and risk for severe adverse events (grade 3/4).
The combination of ipilimumab plus nivolumab is associated with a higher clinical response rate than nivolumab or pembrolizumab alone that, in turn, are more effective than ipilimumab monotherapy. However, the risk of grade 3/4 immune-related adverse events is greatest using the combination of ipilimumab and nivolumab, less with ipilimumab alone, and even lower when using nivolumab or pembrolizumab as monotherapy, Dr. Bolognia says.
RELATED: Nanovaccine shows promise for melanoma
The most common cutaneous side effects associated with the immune checkpoint inhibitors include pruritus, lichenoid dermatitis, morbilliform and eczematous eruptions, and vitiligo-like leukoderma. Interestingly, bullous pemphigoid as well as sarcoidosis have also been observed.
MANAGING IMMUNE-RELATED ADVERSE EVENTS
In 2018, guidelines for the management of immune-related adverse events in patients treated with immune checkpoint inhibitors were published in the Journal of Clinical Oncology.1 The skin toxicities were divided into three categories:
- rash/inflammatory dermatitis,
- bullous dermatoses, and
- severe cutaneous adverse reactions (e.g. Stevens-Johnson syndrome, toxic epidermal necrolysis, drug reaction with eosinophilia and systemic symptoms).
The recommendations for management were based on severity grade and generally consisted of increasing the intensity of systemic corticosteroid treatment as severity increased, in addition to drug holidays. However, there are other interventions that dermatologists can offer, Dr. Bolognia says.
“Rather than initiating oral corticosteroids to manage a grade 2 lichenoid, eczematous or psoriasiform reaction, acitretin, apremilast or methotrexate can be considered,” she explains. “Similarly, whereas the guidelines recommend initiating an oral corticosteroid to treat a grade 2 bullous pemphigoid eruption, oral doxycycline with or without nicotinamide can be administered instead.”
Importantly, patients with melanoma who develop immunotherapy-related cutaneous adverse reactions, in particular vitiligo-like depigmentation, have been shown to have an improved survival. However, it is important to distinguish whether the vitiligo-like depigmentation (“leukoderma of melanoma”) is spontaneous or treatment-related.
RELATED: Imaging evolves to guide Mohs surgery
“If the leukoderma is spontaneous, the patient needs to be restaged even though it is not always a reflection of metastatic disease,” Dr. Bolognia says.
Disclosures:
Dr. Bolognia reports no relevant conflicts of interest to disclose.
References:
1. Brahmer JR, Lacchetti C, Schneider BJ, et al. Management of Immune-Related Adverse Events in Patients Treated With
Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol.
2018;36(17):1714-1768.














 premarket notification")
Newsletter
Like what you’re reading? Subscribe to Dermatology Times for weekly updates on therapies, innovations, and real-world practice tips.

















